I have written two posts comparing the COVID-19 situation in Sweden and Denmark (see here and here). I find the comparison useful, because they are very similar countries in the same basic region of the world, but they had remarkably different responses to the disease. Sweden initially avoided lockdowns and tried to target their social restrictions, while Denmark followed the practices of most other countries, strongly limiting what their citizens could do during the pandemic. Sweden thought that if they allowed the disease to run its course among those who are not at high risk, they would achieve herd immunity, and the disease would lose its impact. As a result, they tried to target their severe restrictions to those who were at high risk, allowing the rest of the population to live life more normally.
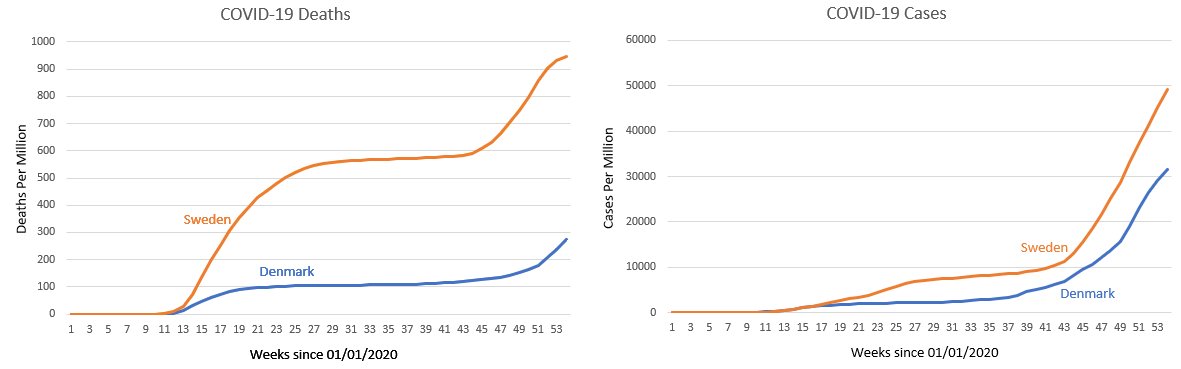
By fall, there were those who thought the strategy had worked. Case rates were falling, and Sweden seemed to have weathered the storm. However, in my August post, I said that Sweden had not reached herd immunity, and it turns out that I was right. If you look at the above graphs (data from the European Centre for Disease Prevention and Control), you will see that while both Sweden and Denmark saw a leveling off in the summer and early fall, COVID cases and deaths quickly shot up later on. To date, Sweden’s COVID-19 deaths per million are more than three times that of Denmark’s, and right now, there is no indication that either country will see a slowdown in cases or deaths, at least not until the vaccines are widely distributed.
Now please understand that comparing two different countries is fraught with peril, and even though Sweden and Denmark are similar in many ways, we cannot use these data to definitively say that government-imposed lockdowns are responsible for the difference. Indeed, there is a fairly recent study that tries to compare different countries, and they conclude that while some social restrictions did reduce the spread of the disease, severe restrictions (like lockdowns) didn’t help at all. Interestingly enough, they use Sweden as part of their baseline for countries that didn’t implement severe restrictions, but they do not use data from Denmark in any way. I personally think their analysis uses countries that are just too different to be compared in any meaningful way.
To show you what I mean, I added the U.S. and Italy to the graphs above to show you where they fit.
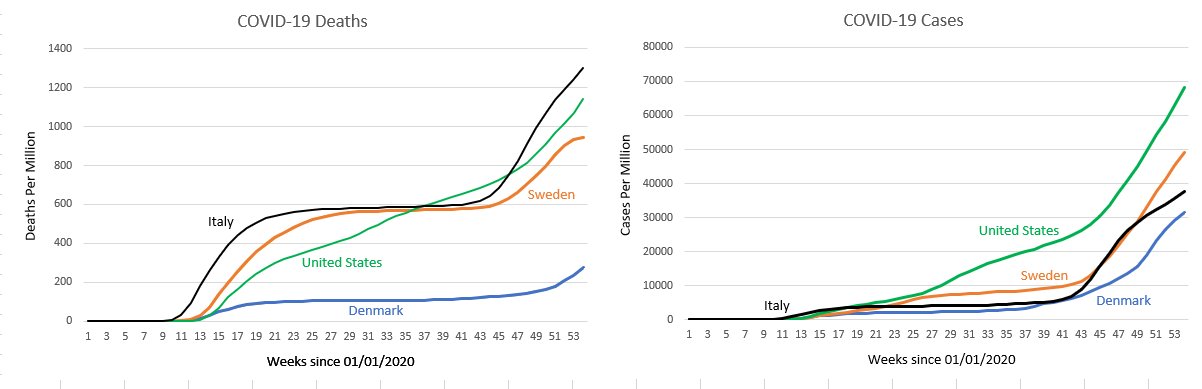
Notice that while the general shape of Italy’s death graph is similar to that of Sweden and Denmark, the U.S. deaths look very different. Conversely, when it comes to cases, the U.S. graph has the general shape of Sweden and Denmark, while Italy is different. Finally, notice that the total number of deaths per million varies by nearly a factor of five, despite the fact that three of the four countries on the graph had strict limitations on what many of their citizens could do.
I think there is one firm conclusion we can make from the data presented above: Sweden’s strategy of trying to control the disease using herd immunity acquired through exposure did not work.
This makes sense from a narrow epidemiological perspective. But when I think about whether broad policy decisions on an epidemic are “working,” I consider it only a partial answer whether deaths are going up or down. To create a simple hypothetical: if a given policy resulted in X deaths from Covid and great disruption to society, is that better or worse than 2X deaths and minimal disruption? 3X? 4X? There’s not a right or wrong answer to that question. Our society regularly tolerates additional deaths to gain some benefit, sometimes even for what might sound like a petty reason (we have 70 MPH speed limits on highways just because then we can save time by going fast, instead of dropping it to 30 MPH which would probably eliminate almost all highway deaths; we’re ok with some people dying merely because we’re impatient).
Sweden’s policy may have resulted in more deaths.* But I think that’s a different question from whether, in a broader sense, it “worked.” As Thomas Sowell put it: “There are no solutions, there are only trade-offs.”
* (And this raises even more questions, though. We’ll all die, so no policy really avoids death; it just delays it. So then…are the people dying now people who were very likely to do soon anyway? Does that mean there could be a drop of deaths in 2021, when those people who would have died then can’t, because they already died in 2020? I think most policy considerations do treat the death of an 80-year-old with multiple co-morbidities different from the death of a healthy teenager. So many variables and unknowns right now.)
Yes, but in terms of their strategy, it didn’t work. Their strategy was to stall the disease by achieving herd immunity. That clearly didn’t happen. When it comes to whether or not Sweden made a better overall decision than Denmark, you are absolutely correct. We can never know, because there are too many tradeoffs to consider.
Yes, completely agree. But I guess that’s my problem with how the policy makers, epidemiologists, and (to a large extent) public have defined success. My criticism is with their goal of “stalling the disease” with no other parameters. It should have been, “We’re fine with 3x the number of deaths as Denmark if that allows people to live their lives.” Then we could say they were successful. Or if they had said, “We’re ok with 2x, but not 3x,” then we could say they were not successful. By focusing only on deaths but not considering all the negatives of restricting society, their policy calculations were wrong from the start. In other words, my comment is that the problem is at the beginning, when someone decided it’s herd immunity or bust. Now it will be nearly impossible to have a conversation about success, since the goal posts started in the wrong place.
From my understanding and I have been following them since the beginning of all this. They knew there would be deaths, but they implemented a plan that would go as easy on the economy as possible. The epidemiologist in the beginning stated that the projections given were way out to lunch and that they were not destroying the nations economy on that projection. So for anyone to be talking about the deaths is a mute point because they knew they would have deaths among the elderly and ill populations. They did conclude that they would not be getting the “2nd wave” to the extent that countries with lockdowns would.
But their plan was predicated on the belief that they would acheive herd immunity. Since they are definitely experiencing a second wave similar to other countries (and worse than Denmark), that clearly failed. I agree that deaths and cases are not the only measures of whether or not a country responded properly to the pandemic. I am just saying that the idea that they could reach herd immunity through exposure has been demonstrated to be wrong.
Okay but it is also clear that once a person gets the virus that they get strong immunity against that family of viruses. So it could be possible that herd immunity is existing to a percentage of the population, but also that Sweden has a large elderly population, compared to Denmark. Italy for example has a huge elderly population, and a large percentage are smokers. Does Denmark eradicate it’s elderly by euthanasia? If so, that would definitely contribute to the lesser deaths because as we know covid mostly kills 80 years plus people, with multiple morbidities at that. For example Greenland aborts all babies who appear like they might be down syndrome. Greenland just a few years ago had one baby who was “accidently” born with down syndrome. Countries in Africa don’t have the same death stats as Europe or western countries because they have large population of younger people and their elderly aren’t propped up in senior homes deteriorating on doctors drugs. So there are multiple scenarios that could affect those graphs you have. But to zero in on the herd immunity issue. It is a well known fact that immunity comes from contracting a virus, and for that reason, because we know a virus on the earth behaves like a virus on the earth, that herd immunity will eventuate. I had recently read on the CDC website that if you were born 1959 and before you never need a German Measles vaccine/booster. The reason for that is they were pre-vaccination days and everyone just got the childhood diseases and gained “lifelong immunity”. Now, boosters are needed more and more often for German Measles.
Yes. Once you get it, you have immunity. However, “herd immunity” means something very specific. It means the virus cannot spread through the population because a large enough percentage of the people are immune. Sweden clearly doesn’t have that, because they have a second wave that is similar to the other countries. Yes, populations from each country are different, so comparing countries is fraught with peril. However, we know that Sweden’s strategy of stopping the virus with herd immunity failed miserably, because the virus is still spreading through the population. Thus, there is no herd immunity. There are individuals who are immune, but not enough of them to keep the virus from spreading.
Okay I agree. But is there a time frame in which the virus must reach herd immunity? I don’t recall there being a time frame, except that they thought their second wave wouldn’t be as strong as the surrounding countries. That could be a time frame. But we have limited data. Because perhaps Sweden’s elderly became foot loose and fancy free and are solely responsible for the heightened 2nd wave? It would be good to know what caused the spike because we always have viruses around and are always gaining immunity as we live.
There is no time frame. Herd immunity is defined as when immunity is so common that the virus can no longer spread. It doesn’t matter how long that takes. However, in this case, the idea was to reduce the spread of the disease until a vaccine was made available. Sweden thought that allowing the low-risk people to be exposed would do that via herd immunity, and that didn’t work. Yes, there are many possible reasons for the death rate spiking, but there would be no increase in death rate if the virus was not spreading, so regardless of the cause, the fact that people are still getting (and dying from) the disease means the herd immunity strategy failed.
Dr. Wile,
I had not read your post just yet (its on my list), but just saw this and thought I’d let you know: https://twitter.com/FatEmperor/status/1351860543485857792
Seems compelling and simple enough, huh? What might be missing? 2021? : )
+Nathan
Except that it’s simply not true. Like it was in the U.S., 2020 was the deadliest year on record in Sweden. Here’s another way to see that.
Okay but when you talk about deadliest on record. When a country does lockdowns and brings the economy to a grinding halt do you not think that this becomes deadly? For example our town of 25,000 has had zero covid deaths, yet from my knowledge there have been about 13 people have committed suicide because of covid, and not from covid. And that is just my knowledge. the news is mum on the issue and they keep it quiet. So when we are looking at deaths, we should right alongside those covid deaths have the suicide chart going too. And lets include the ages of the dead people from covid, and because of covid suicides. The herd immunity result might be a lot clearer sometime later.
Of course lockdowns also cause deaths. However, you can’t blame lockdowns when it comes to Sweden, since they didn’t do lockdowns. So with lockdowns, this is the deadliest year on record in the U.S. and without lockdowns, it is the deadliest year in Sweden. While comparing countries is fraught with peril, I think this indicates that lockdowns aren’t the major cause of the excess deaths. Once again, however, this has nothing to do with herd immunity. That result is already clear. Sweden did not reach herd immunity. We know that because the virus is still spreading rapidly there.
Dr. Wile,
Thanks for replying to me. Well, yes, that is quite different. Why the glaring different in viewpoint? Do you think the tweet is showing just “another way to see” the evidence or is not even really being statistically honest at all? It would seem like it must be the latter….
+Nathan
The data being presented are wrong, plain and simple. The person who produced the presentation might have made an honest mistake, or that person might have been deliberately dishonest. I have no idea. However, I do know that the presentation is utterly false.
Hi Dr. Wile,
I want to get your thoughts about the use of fetal cells during the testing phase of the Moderna and Pfizer Covid -19 vaccine? I just learned about HEC293 and the role of these cells in vaccine development. As belivers, can we take these vaccines in good conscious?
Reference:
https://www.health.nd.gov/sites/www/files/documents/COVID%20Vaccine%20Page/COVID-19%20Vaccine%20Fetal%20Cell%20Handout.pdf
Yes, we can. First, the abortion that produced the HEK293 cell line occurred almost 50 years ago. The child is dead regardless of what happens to his or her cells. Thus, the use of the fetal cell line in the initial testing phase of the vaccine development process has not contributed to the death of any child and did not cause the number of abortions to change in any way. I would agree with Brian Kane, senior director of ethics for the Catholic Health Association of the United States, who is quoted in the link you gave. He makes a distinction between a medicine that requires the use of fetal cells in production as compared to the Moderna and Pfizer vaccines, which used them only in initial proof-of-concept experiments. His full quote is:
Second, this (and other) fetal cell lines are used in all sorts of research that has led not only to treatments for disease, but also basic information about biology. If you don’t want to utilize any medicine that has benefited from the use of fetal cells, you probably have to restrict yourself to medicines produced with biological knowledge and techniques that existed only before the 1990s.
Third and most importantly, I cannot fathom how it is “pro life” to let people die of an infectious disease today in order to protest a single abortion that took place almost 50 years ago. This is why most pro-life organizations (including the Roman Catholic church) support the use of vaccines which use fetal cells as a part of the production process when there is no alternative. As the Vatican Statement on the issue says:
In other words, if a vaccine that has never used fetal cells is available, you should use it instead of one that used fetal cells. However, if no alternative exists, it is better to save lives in the present than protest murders from the past.
Thanks for your response and thoughts, Dr. Wile. My family and I have immensely appreciated your Covid-19 and vaccine related posts during these times.