Over the past few weeks, I have gotten some emails regarding COVID-19 that were filled with misinformation. In an attempt to clear up this misinformation, I thought I would look at some data that are rather easy to obtain and analyze: total deaths in the U.S. over the past seven years and the deaths attributed to COVID-19. They come from the CDC, which I know many of my readers don’t trust. Indeed, I don’t trust the CDC when it comes to many of their recommendations, including some related to COVID-19. Nevertheless, these data are rather hard to manipulate, since they come from many independent sources. Thus, while they might not be 100% accurate, the overall conclusions we can draw from them should be reliable.
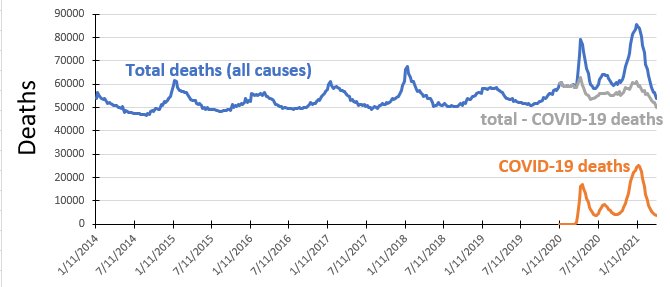
Looking at the above graph, then, what do we see? Let’s start with the total deaths (in blue). They follow a familiar pattern in the five years leading up to 2020. They peak in January, trail off in the summer, and start rising again in autumn. The peaks are generally attributed to two things: cold weather is more deadly than warm weather, and the influenza season typically peaks in January/February. Indeed, if you look at the heights of the peaks in the years before 2020, you can see when the more severe influenza seasons were: 2015 and 2018.
Notice, however, that 2020 and 2021 break the pattern established in the previous years. The peak in 2020 is much, much higher than the peaks in the previous years, and it comes later in the year (mid-April). In addition, when it comes back down to its minimum (late June), it is much, much higher than the minimum of any other year. Then, there is a bump that occurs later in the year, followed by another peak that is even higher than the one in April of 2020. Clearly, this tells us something unusual happened in 2020, and it is still happening in 2021.
Of course, we know what that unusual situation is: COVID-19. If we graph just the deaths attributed to COVID-19 (in orange), you see the same unusual pattern: a peak that occurs in April of 2020, another bump, and then an even larger peak. Just to see how much of this unusual pattern can be attributed to the COVID-19 deaths, the gray line shows you what happens when you take the total deaths and subtract the COVID-19 deaths. The result is something that looks a lot more like the pattern that was established in the past seven years. However, the pattern isn’t exactly the same as what is seen in the previous years. Notice that the gray line never gets as low as the blue line does in 2014-2019. Thus, even after subtracting out the COVID-19 deaths, there are still more deaths than in the previous years.
What does all this mean? Well, let’s start with two things we can say for certain. First, contrary to what you may have heard (and what I was sent in email), COVID-19 is NOT just a severe flu-like disease. It is responsible for more deaths than any flu in the past seven years. Indeed, the only influenza that was more deadly than COVID-19 in the U.S. (as of right now, anyway) was the 1918 Spanish flu. Second, COVID-19 deaths are not being significantly over-reported. If that were the case, subtracting out the COVID-19 deaths would have resulted in fewer deaths than in previous years (the gray line would have dipped lower than the blue line dips in previous years).
What can we say about the fact that even after subtracting out the COVID-19 deaths, there are still more deaths in 2020 and 2021 than the previous years? As I see it, there are two possibilities. It’s possible that COVID-19 deaths are being under-reported. It’s also possible that the COVID-19 measures that have been instituted have produced some deaths as well. I think the second option is more likely. Social isolation, delaying doctor appointments, etc., will result in more deaths. However, the number of those deaths is small compared to the COVID-19 deaths.
There is one more thing that I see in the data, but it is preliminary at best. Notice that the peak occurred much sooner this year than last. While the peak number of deaths in 2020 occurred in April, this year’s peak occurred in January. Assuming the virus hasn’t changed substantially over the past year, that means something happened to curtail COVID-19 deaths. What happened between 2020 and 2021? The vaccine started rolling out. The first doses were given in December of 2020, and the initial focus was on health care providers and those who are most at risk of dying from COVID-19. To me, it isn’t surprising that this produced enough of a slowdown in COVID-19 to cut the peak back three months. Once again, that is a preliminary conclusion which could be wrong. However, I do think that time will bear it out to be true. Regardless, I will post a similar analysis in a few months to see what the data say then.
Thank you Dr Wile. I dont have strong feelings about this one way or another but I do feel anxious when I hear others talking about this topic if covid vaccine. Your blog about it gave me some peace. Praying for you and yours well being.
I will just add that in several states, Pa and NY being two of them, decisions made by governors resulted in THOUSANDS of Covid deaths that otherwise wouldnt have happened. They forced sick patients back into nursing homes, which quickly decimated those populations. So while I agree that Covid is bad, we dont actually have a case for HOW bad it is, given that fact. Also, many people were declared to have died from Covid, who likely didnt…I personally know several who were deemed covid deaths, but weren’t. So it’s all muddy and hard to really get any kind of clear and accurate data from.
But these data help clear up that confusion. As I show, the COVID-19 cases can’t be severely overreported, since once you subtract them out, the number of deaths are still higher than normal. Thus, while I am sure there are some COVID-19 deaths that were not really due to COVID-19, these data show that they aren’t significant. Also, while you are right that there were lots of needless deaths in nursing homes because of irresponsible governors, the data indicate that the majority of COVID-19 deaths were not from nursing homes. So I don’t think the situaton is very muddy.
Could it be that the initial peak in April is due to when the virus was first being introduced into the population (March) but the January peak shows Covid-19 beginning to take on a more seasonal pattern like the flu?
The problem with that interpretation is that COVID-19 isn’t an influenza virus. If it has a seasonal pattern, you would expect the pattern to resemble what we saw in 2020, with the deaths trailing of much later than the flu. Of course, there are a lot of unknowns, so I guess we can’t rule out a new seasonal pattern. However, the next few months’ worth of data should be revealing.
The majority of COVID-19 death may not have been from nursing homes, but 40% were. It’s not the majority, but it’s still a pretty high percentage. But if you took the Covid deaths on the graph and lowered them by 40% (and of course that would be assuming that nobody in any nursing home had died of Covid, which is unlikely), the two Covid death spikes would still be higher than the third highest death spike in the last 7 years, which was the influenza spike in 2018.
What were some of the independent sources the CDC used to make this graph?
The CDC simply aggregates the data. Each death is certified locally by a medical institution. Technically, then, all the data are independent of the CDC, since the CDC doesn’t do any death certification. Each state has an indepedent database of deaths (usually by county), which can be used to make sure the death statistics compiled by the CDC are accurate.
Do you have data on deaths related to the isolation during quarantine, such as suicide? If so, could that account for the higher than normal gray portion of the curve after COVID19 deaths were subtracted?
I don’t have that kind of data, but you are probably right.
Hello Dr. Jay! How are you?
Do you think ivermectin is effective against Covid – 19? I’m pretty skeptical about the effectiveness. And I found a study which seems to vindicates my point.[1]
https://jamanetwork.com/journals/jama/fullarticle/2777389/
God Enlighten you!
The report you link says that ivermectin is ineffective against mild COVID-19. There have been several studies, and they generally indicate that there is some positive effect, especially if treatment is started early:
https://ivmmeta.com/
Interesting! I guess my aunt will be partially happy about it(partially because she doesn’t want to take the vaccine, and the authors of the study you linked do not approve her behavior).
God Enlighten you!
Hi there, Dr. Jay!
How can I explain to people that the mDNA vaccines for Covid 19(like Pfizer) isn’t going to alter your DNA?
God Bless You!
I discuss that here.
This is a little off-topic, but can you comment on the idea of virus shedding? You’ve probably heard the claims going around that someone who has been vaccinated with any Covid vaccine is now creating and shedding variants of the virus and passing them along to those who are unvaccinated. I have read claims of menstrual irregularities and infertility among unvaccinated women who have been around someone who has been vaccinated. Additionally, can you remark about the death rate among people who have been received a Covid vaccine? I’ve read that the Covid vaccine death rate is higher than the death rate of all other vaccines combined. I’ve tried researching on the CDC and VAERS websites but have had difficulty using the sites. Thank you.
It is impossible for people to shed the virus from the vaccines that are currently approved. The Moderna and Pfizer vaccines don’t use the virus or any part of the virus, so there is nothing to shed. The Johnson&Johnson vaccine uses a strand of DNA from the virus, but it is combined with a different kind of virus (an adenovirus, which is a common cold virus). Thus, even if you shed a virus from that vaccine, it wouldn’t be the virus that causes COVID-19. It would be a cold virus.
There is absolutely no truth to the idea that the COVID-19 vaccines are deadly. Through January 13th of this year, more than 13 million doses of the vaccines were administered. Only 113 deaths were reported to the VAERS, and the causes of death did not suggest any relationship to the vaccine. This is one of the many sources of misinformation that occurs with all vaccines. The VAERS simply compiles all adverse events that occur after vaccination. It DOES NOT record adverse events caused by the vaccination. The VAERS is simply used to compile any adverse effect that occurs after vaccination, whether or not it was caused by the vaccine. Those data are used to then investigate further, to see if any of the adverse effects were caused by the vaccine or simply happened by chance. After all, with millions of doses being given, there are bound to be thousands of adverse effects that occur afterwards by coincidence alone. So far, the data indicate that those deaths would have happened with or without the vaccine.
This scientist, French Virologist and Nobel Prize Winner Luc Montagnier would beg to differ with you.
https://rairfoundation.com/bombshell-nobel-prize-winner-reveals-covid-vaccine-is-creating-variants/
And I would say the data beg to differ with him. The U.S. data show a steady decrease in both deaths and infections correlated with the vaccine rollout. Worldwide, cases and deaths went down in January, back up in March, and then down again in April. However, vaccine distribution has been very spotty worldwide. In countries where the vaccine is being distributed effectively (France and the UK, for example), cases and deaths are going down.
I think Israel is a good case study for the vaccine, since a high percentage (over 60%) of the people have received at least one vaccine. If you look at a graph of Covid deaths in Israel over time (Google “Israel covid deaths”), you can see that deaths have sharply declined since the vaccine was first distributed. I would think this is the opposite of what we would expect if the vaccines were truly causing ADE, as that article claims. What are your thoughts on that, Dr. Wile?
Yes. That’s probably the best case study which shows Dr. Montagnier is incorrect.
Thank you for commenting on the idea of virus shedding. I’ve been skeptical about that since I first heard about it.
The link you provided shows data only through January. I am wondering why I cannot find a more recent report. I have heard the death total for people who have received the vaccine is now higher than 4,000. I am just having difficulty finding anything concrete.
Technically speaking, the vaccines are not approved, right? They are available for Emergency Use Authorization which was only able to happen if no other treatment methods were available. Ivermectin, Hydroxychloroquine, and monoclonal antibodies have all been effective in many cases. I understand that not all patients are candidates for those treatments, but plenty of people are. To dismiss those therapeutics in order to push a vaccine through seems very unethical. Possibly many lives could have been saved if those treatments were not rebuked.
Once again, the deaths reported to the VAERS are not vaccine-related deaths. There have been more than 4,000 deaths reported to the VAERS at some point after vaccination, but none of them have been definitively linked to any vaccine. Right now, the only vaccine that might have caused any deaths is the Johnson & Johnson vaccine, and they are very rare (if at all). As the CDC says:
When millions of doses of the vaccines have been given, there will be thousands of deaths by coincidence alone. If the vaccines were killing thousands of people, why are the deaths in the U.S. going down?
The vaccines have been approved for emergency use. They have been put through rigorous clincal trials and are being monitored for safety, as the link above indicates. The only reason they needed emergency use authorization is that the timeline was shortened because of the severity of the pandemic.
Ivertmectin and hydroxychloroquine have moderate effectiveness, depending on when they are given. Antibody treatments are more effective, and like the vaccines, they have been been approved for emergency use. None of these treatments have been “rebuked.” They are being used when the doctors treating the patient think that they will be effective.
No one is pushing the vaccines over these treatments. The vaccines play a completely different role. They do not treat the disease. They prevent it. They are one part of the complete strategy being used to fight the disease.
Jay, that is utterly false, there isn’t a shred of evidence they prevent transmission, in fact the Pfizer primary literature flat out states this technology was not designed to prevent transmission. You don’t need to read past the abstract to find that statement.
You definitely need to read past the abstract. These vaccine allow you to fight off the virus before it develops a load that is high enough to cause you to get ill. In turn, that helps reduce transmission, because people with lower viral loads are much less likely to transmit.
Are you familiar with Dr. Peter McCullough? I also follow America’s Frontline Doctors. All of these doctors have very serious concerns regarding the Covid vaccines. https://rumble.com/vhrbej-covid-vaccines-risks-benefits-and-safety.html?fbclid=IwAR2nA2ty-638BHktx7RRNmyKVypcaTuxxC5vDlX2-GTjnmDprLozLFDELtg
I am familiar with both Dr. McCollough and America’s Frontline Doctors, and I have to say that they are not being very honest. In the video you linked, for example, Dr. McCullough references a study from Norway that investigated deaths that occurred after the vaccine. He says the report found
However, the actual article says something QUITE different:
This is the problem with doctors who promote their own agenda instead of looking at the data. The VAERS deaths do not give you any idea of the deaths related to the vaccine. Millions of doses are given, and hundreds die every day. By sheer coincidence alone, there will be lots of deaths right after a vaccine. Thus, we must use studies to determine whether deaths are coincidental or caused by the vaccine. Right now, the evidence points to few (if any) are related to the vaccine. This is bolstered by the fact that deaths are not going up. Instead, as the data show, they are decreasing. If the vaccine were causing a lot of deaths, then that wouldn’t be happening.
Pinz, to add to what Dr. Wile said, a lot of preliminary data so far suggest that the Covid vaccines do reduce the likelihood of transmission. This study shows that when Israel began vaccinating their elderly, the infection rate among the elderly dropped, even though the infection rate among the younger population did not change much:
https://www.nature.com/articles/d41586-021-00316-4
An observational study in Israel found the vaccine caused a 75% reduction in infection: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)00448-7/fulltext
And as Dr. Wile pointed out, studies are showing that a lower viral load reduces the likelihood of spreading the coronavirus to others (https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30985-3/fulltext) and that vaccination reduces the viral load (https://www.medrxiv.org/content/10.1101/2021.02.06.21251283v1).
I am so glad I stumbled across your site! Thank you for your analysis of the Covid-19 deaths vs. total deaths. So many secular sources have been pushing getting vaccinated so hard that I began to think it was from Orwell’s Ministry of Truth. I heard the message the first time, I don’t need to hear it again on every commercial break. Having a detailed analysis that shows that the Covid-19 deaths are going down likely due to the vaccines’ availability makes me feel better about getting one. However, as I am not in a high risk category, and won’t be traveling until next year, I may opt to wait for the Novavax vaccine (It’s supposed to come out in the fall of this year). To my knowledge, the Novavax vaccine doesn’t use aborted fetal tissue in any stage of the development or production of the vaccine, whereas the Pfizer, Moderna, and Johnson & Johnson vaccines do. The J&J vaccine is particularly bad in this regard, because the aborted fetal tissue is used in the production of the vaccine, not just the development like Pfizer and Moderna. However, when I started to dig a little deeper, I found out that at least one of the aborted fetal tissue lines came from an 18 week gestation (!!) fetus in the 1980s, and another, the 1970s? First, yuck. Second, how is it possible that aborted fetal tissue can survive that long? I’m assuming the cells are being made to replicate somehow? Third, why is the aborted fetal tissue so attractive to these companies for development and production of vaccines, versus other kinds of human tissues? If you have insight into this, I would be grateful.
The Pfizer and Moderna vaccines do not use fetal cells in their production. In fact, they don’t use any cells at all. Fetal cells were used in a one-time series of tests to determine whether or not the mRNA would be taken into a human cell, but there are no fetal cells used in the production of those two vaccines. The Novavax is similar. Tests were done on fetal cells, but they are not used in the production. Fetal cells are used in the production of the Johnson & Johnson vaccines.
It is important to note that whether or not you get a vaccine that uses fetal cells in the production, it doesn’t affect the number of abortions done in any way. This is because, as you note, the cells used are from long-ago abortions. Remember, cells reproduce, so the cells are kept alive, allowing them to reproduce so that they can be used over and over again. This is called a “cell line,” and there are thousands of human cell lines being maintained. Some are from abortions, others are from adults. Fetal cell lines are attractive because they have been around for a long time and have been well-studied. Thus, the cells themselves are well-understood, which helps in any scientific endeavor that uses cells. In some vaccines, the virus is so specific that it is very difficult to grow it on anything other than human cells, and since the fetal cells are so well-understood, those are the ones typically chosen.
Much of the biological knowledge we have about human genetics, how human cells work, how human cells respond to outside sources, etc. was discovered using fetal cell lines. I can understand why you would be hesitant to accept any medical advance made using them, but please understand that virutally EVERY modern medicine exists because of them – either because they were used in some phase of the testing process or because the medicine makes use of knowledge discovered from those cells. I don’t have a problem with them, because their use doesn’t affect the number of abortions done in any way. As a result, any life-saving advance that they have given us is a silver lining in the cloud of the baby’s murder. Once again, however, I can understand those who avoid medicines that use them.
I appreciate all that you are doing and I have read your article and the comments. I am flip-flopping everyday with this topic. It sounds like we should all get vaccinated and numbers are getting better because of it. But, then I hear about problems with the vaccine and am worried about myself and my family being vaccinated. Just last week I heard that our friend’s daughter who is not vaccinated but working with vaccinated people is experiencing weird cycles with her period. I know that it could be a coincidence, but then another person we know has experienced extreme pain and headache after her second vaccination. Then there is this article,https://www.youtube.com/watch?v=Du2wm5nhTXY by scientific people talking about problems showing up with the vaccine. I’ve seen others commenting as well , who are well known in the medical community. Why would they be spreading lies? What benefit is it to them? And why are there no other side effects reported to us other than blood clots. Where is the truth? Please help me Jay. I’m not a doctor or a scientist but how do I dismiss all these claims. Here’s another video that is really radical. https://banthis.tv/watch?id=60a59596eb541a3957bddf33&fbclid=IwAR25EADKaR3p8VX88hNPdesMQGM75zOPOzUALDNg9LTHLVIVAaXCPyXN5_A
I have no idea whether these people are lying or just spreading false information. There is a difference. Nevertheless, they are saying things that are completely false. For example, Dr. Malone is not the inventor of mRNA vaccine technology, as the video claims. While at the Salk institute, he did investigate how to put RNA into a cell, but the technology of the vaccine is utterly different from what he did. At the time, dozens of researchers were doing the kinds of research he was doing, so if he is the inventor of the technology, dozens of others are as well. They say the spike protein is cytotoxic, but there is no evidence of that. Indeed, if it were, you would see the effects showing up in the vaccinated population more than the unvaccinated population, and they are not. Also, they don’t seem to understand the spike protein generates antibodies that….destroy the spike protein. This is why studies show that the spike protein becomes undetectable in the body 14 days post injection.
You are hearing about blood clots as a side effect because right now, those are possibly related to the vaccine. You are also hearing about heart inflammation in the young, because that is also possibly related to the vaccine. In all other cases, the adverse effects that have been reported are not any more frequent in the vaccinated population than the unvaccinated population, based on the studies that have been done so far.
The second video is utter nonsense. It is simply not possible for such nanotechnology to be in the vaccine. That kind of technology doesn’t exist yet in injectable form.
Thank you for taking the time to check out these videos.
I saw that video with Dr. Malone a couple weeks ago and thought it was odd that they were saying he was the inventor of mRNA technology. Where does Katalin Karikó fit in? Was she the pioneer of the mRNA technology?
There was no single pioneer in this technology. This timeline (from an article in Nature) shows that:
Key discoveries and advances in the development of mRNA as a drug technology
The box above 1989 represents Malone and two others’ contribution (Development of cationic lipid-mediated cationic delivery). The box below 1990 also contains his and six others’ work. The box above 2005 (Discovery that nucleoside-modified RNA is non-immunogenic) is Karikó’s and three others’ main contribution. Essentially, Malone and his colleagues were the first to get mRNA into a cell and show that it could be translated into a protein. However, that didn’t lead to anything effective, since the body attacks such mRNA, degrading it. Karikó and her colleagues showed how to keep that from happening. That’s why some sources claim she is the inventor. Without her and her colleagues’ discovery, there would be no vaccine today. However, as the timeline shows, that can be said of many other scientists. Neither Malone nor Karikó were the main pioneers, as there were no main pioneers. There were dozens, each of whom made critical contributions along the way.
One other thing that is important to note. Malone claims to be the “inventor,” but he never bothers to include the other seven who were a part of the two contributions with which he was involved. If Malone is the “inventor,” why aren’t those others also “inventors?” Contrast that to Karikó, who put together this timeline, along with two others who are working in the field. All three of them hold patents in this technology. Nowhere in the paper do they lay claim to being the “inventor” of the technology. Nowhere do they list a main pioneer. That’s because there is none, and if Malone were being honest, he would admit that as well.