
 So far, I have written three articles about how horrible social media is as a source of scientific information (see here, here, and here). Facebook might be a great way to find out what your friends are eating, but it is one of the worst places you can go to learn about science, especially the COVID-19 pandemic. That’s because lots of people (left, right, and center) have decided to politicize the pandemic, and the unscrupulous among them have transformed science from its true nature (a very imperfect mode of inquiry) into a weapon. Unfortunately, many people don’t recognize weaponized science, and as a result, they tend to share things that fit their political views, regardless of whether or not they are accurate.
So far, I have written three articles about how horrible social media is as a source of scientific information (see here, here, and here). Facebook might be a great way to find out what your friends are eating, but it is one of the worst places you can go to learn about science, especially the COVID-19 pandemic. That’s because lots of people (left, right, and center) have decided to politicize the pandemic, and the unscrupulous among them have transformed science from its true nature (a very imperfect mode of inquiry) into a weapon. Unfortunately, many people don’t recognize weaponized science, and as a result, they tend to share things that fit their political views, regardless of whether or not they are accurate.
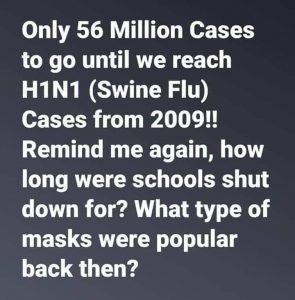
Consider, for example, the statement shown above. I have seen it on my Facebook feed at least a dozen times. While the statement is factually accurate, it supports a false narrative. Yes, there have been roughly 4 million cases of COVID-19 in the U.S. so far, and there were estimated to be 60 million cases of H1N1 during the 2009 pandemic. So the H1N1 pandemic of 2009 was “worse” than the COVID-19 pandemic today. Therefore, all the precautions we are taking against COVID-19 (shutting down schools, wearing masks, etc.) are just a result of politicians trying to use the current pandemic to their advantage. Of course, that’s simply not true. The reason we are taking precautions against COVID-19 is that it is significantly more deadly than H1N1. Out of the estimated 60 million cases of H1N1 in 2009, there were only about 12,500 deaths. Out of the roughly 4 million cases of COVID-19, there have been almost 150,000 deaths. Since 15 times fewer cases have produced more than 10 times as many deaths, it is easy to understand why we are taking more precautions against this virus!
Just to give you one more example, yesterday I saw this statement on my Facebook feed:
The COVID-19 death rate without a vaccine is lower than the flu death rate with a vaccine.
As far as I can tell, there is no way you can massage the data to make that statement even factually correct. For the 2018-2019 flu season, there were estimated to be more than 35.5 million cases and 34,200 deaths. Once again, for the current COVID-19 pandemic, there have been roughly 9 times fewer cases, but about 5 times as many deaths.
Now please understand that I am certain the number of COVID-19 deaths are being overreported. But they aren’t being overreported to the point where you can conceivably compare this current pandemic with the H1N1 pandemic of 2009 or the seasonal flu. In the same way, I know that politicians are using this pandemic to their advantage, but that doesn’t mean it isn’t real and isn’t serious.
So when it comes to getting information about the pandemic, choose your sources wisely, and do not include social media on the list!
Do you think that the high number of deaths can be contributed to the fact that the treatment they used to help the patients was wrong. For example, putting them on a ventilator made it worse.
That’s certainly possible, but the very fact that so many patients needed ventilators indicates the severity of the virus.
What if they didn’t need ventilators. We were told by government that we need ventilators but the doctors who are experts in the field by no means have consensus on that. The issue was that it was pushed as a treatment and as far as I can tell, there was monetary incentive for hospitals to treat this way. But when people are given less invasive treatment early on there have been better outcomes. Please show me some non political science for why the ventilators were the go to first option in too many cases when the doctors know there are several serious risks involved with intubation and being on a vent.
It is my understanding a ventilator is only used when patients are not getting enough oxygen. I try not to second-guess the physicians treating the patients. Since I am not there and do not have all the data, I choose to believe that the vast majority of physicians would not use a ventilator unless it was their profession opinion that a ventilator was needed. Sure, it’s an opinion, but it’s better than my opinion.
Dr Wile, it isn’t that they were used for patients who had low oxygen, it’s that they were pushed as the only way on Doctors who would normally have started with a much safer option to increase oxygen levels. While I wish I could believe that Doctors are free to use their trained best judgment I know better. Hospitals have protocol for everything. It is the hospital administration that has the power to say what treatment is or isn’t to be used. Doctors who don’t follow protocol lose their jobs. The protocol for covid in the beginning is highly questionable and was being questioned by many doctors.
Maybe change the title of this post to “Please do not get your Covid-19 information anywhere”
https://fee.org/articles/john-ioannidis-warned-covid-19-could-be-a-once-in-a-century-data-fiasco-he-was-right/
Well, you have to get it from somewhere. Otherwise, you don’t know what to do. Yes, it is all a mess, but I think the scientific literature gives the “cleanest” view of the data.
“Needing” ventilators is also questionable. Some yes. But what portion of those was truly “needing”.
https://youtu.be/UIDsKdeFOmQ
Nurse discusses what she saw. And the mis- treatment at her hospital
It is my understanding a ventilator is only used when patients are not getting enough oxygen. I try not to second-guess the physicians treating the patients. Since I am not there and do not have all the data, I choose to believe that the vast majority of physicians would not use a ventilator unless it was their profession opinion that a ventilator was needed. Sure, it’s an opinion, but it’s better than my opinion. This nurse’s report could be 100% true, but I doubt that it can be generalized.
Thanks for posting this information, Dr. Wile. Why do your think the COVID-19 deaths are being overreported? My understanding is that the “probable deaths” are plausibly associated with the virus. Also, I had thought that the “excess deaths” concept seems to support the idea that covid death numbers are properly estimated or even underestimated. What are your thoughts on that?
I am pretty certain they are overreported because if someone has a positive test for COVID-19 and dies, the standard practice is to report it as a COVID-19 death regardless of the actual cause. This makes sense, since COVID-19 could have contributed to the death, even if the cause of death was something like a heart attack. So it’s not a conspiracy or people intentionally inflating the numbers. It’s making sure every possible COVID-19 death is counted. However, that practice will lead to overcounting.
“Excess deaths” are a difficult case to make. As a percent of the total, they are small, so they could just be statistical fluctuations. Also, if there are really excess deaths, they could very well be deaths caused by the lockdown, not deaths caused by the virus. I expect that when studies are done, deaths by suicide will be higher this year, as will deaths by violence and deaths from mild illnesses that were left untreated. Those are all consequences of the lockdown, and they may be larger than the lives saved by the lockdown. We don’t know, of course. I am just saying there are more plausible explanations for excess deaths (if they are real) than undereporting COVID-19 deaths.
Thanks for your explanation. I understand that overcounting is inevitable when using that procedure, but does that necessarily mean that the estimated death count from COVID-19 is actually higher than the true number of COVID-19 deaths? I would think there are other sources of error that would cause some COVID-19 deaths to be missed, such as lack of available testing, false negatives in testing, and deaths at home. With these other sources of error that could result in undercounting, how could we say for sure that deaths are being overreported?
We can’t say for sure, but I would expect that undercounting is the result of random error, while overcounting is the result of an intentional error. In my experience, intentional errors outweigh random errors.
Was this the practice during H1N1, to report it as an h1n1 death just because they died with it though the cause may have been the heart attack? I know more people are also running to get tested, or being sent to because of work than with H1N1. I personally have a friend who was sent due to sinus symptoms to get tested with work. It never progressed but he was in fact positive for Covid 19…so was one of his kids as the other 4 people in the house got tested once his came back positive. The child never presented any symptoms.
It was more common with H1N1 than with the standard flu, at least in 2009. Since it was a pandemic, there was increased testing, especially in hospitals. I suspect it wasn’t as common as COVID-19 testing now, however, since the virus wasn’t as lethal.
https://www.pscp.tv/BreitbartNews/1ynJOqPBaeXKR
Not a huge fan of this source but many people videoed these drs … I also had dinner with a physician who works at the White House … he confirms these doctors testimony … Unfortunately many have died because of them trying to make something political about medicine.
Looks interesting, this started as a suggestion of Doctors without borders, the Clodomiro Picado institute is well known because they develop treatments against snake bites here in Costa Rica:
https://ticotimes.net/2020/07/28/costa-rica-made-plasma-shown-to-inhibit-coronavirus-ready-for-clinical-trials-ucr
That’s great. I look forward to seeing the results of the trial.
Here’s somthing I found on social media you might find interesting
Four scientists from institutions in Canada, Greece and Texas consumed huge amounts of website data for 50 countries and their various government health authorities, such as the the U.S.’s Centers for Disease Control and Prevention, came to this conclusion:
“in our analysis, full lockdowns and wide-spread COVID-19 testing were not associated with reductions in the number of critical cases or overall mortality”
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(20)30208-X/fulltext?fbclid=IwAR0W5TgGhf6PamEUGLQ0cBNjVe-gZNWOBBwXtDTp108Q611ksSHGFK_qFms
I had not seen that. It is odd that they say lockdowns helped the recovery rate, but did not affect critical cases or mortality. The data indicate it – I just find the result odd. I would say that they hit the nail on the head when it comes to the biggest limitation of the study (differences in the epidemiologic curves). Nevertheless, it is very interesting.
Dr. Wile,
Would you please address the safety and effectiveness, or lack thereof, of cloth face masks?
Overall, I think the data show that they are effective, but the effect is small. For example, this study showed that the rate of growth of infections slowed after mask mandates, and the amount by which it slowed increased the longer the mandate was in effect. However, the maximum reduction was still rather small. This study looked at past studies of respiratory viruses in general. They also found that masks had a protective effect. From a safety standpoint, they do reduce blood oxygenation if worn for a long time, but once again, it is a small effect.