It has become so fashionable to blame every calamity on “climate change” that scientists are overlooking REAL environmental issues, like tire waste. (click for credit)
Nowadays, if you want to get funding and become popular in the scientific community, you need to blame any natural calamity you are studying on climate change (aka global warming). For example, salmon populations in the west have been on the decline, and predictably, global warming has been trumpeted as the cause. As one source suggests:
Pacific salmon that spawn in Western streams and rivers have been struggling for decades to survive water diversions, dams and logging. Now, global warming is pushing four important populations in California, Oregon and Idaho toward extinction, federal scientists warn in a new study.
We had determined it couldn’t be explained by high temperatures, low dissolved oxygen or any known contaminant, such as high zinc levels…
Like good scientists, then, they ruled out the “fashionable” explanation and decided to find the real cause. Not surprisingly, they did. They found that urban stormwater runoff could cause the same symptoms that were known to be killing the coho salmon, so the authors painstakingly analyzed the runoff and ran multiple tests.
They identified the chemical that was killing the coho salmon but could not figure out where it came from. Eventually, the researchers found that this chemical was similar to a preservative used in tires, which is charmingly known as “6PPD.” After several experiments, they found that when 6PPD is exposed to ozone and sunlight, it can be broken down into the killer chemical. Thus, the coho salmon are not being killed by today’s favorite boogeyman. Instead, they are being killed by a chemical produced as a result of tire waste.
Now, of course, since the authors of this study seem to be careful scientists (unlike so many that exist today), they are unwilling to generalize their results. Thus, this conclusion applies only to what is killing the coho salmon in the Pacific Northwest. There might be other causes for what is killing the other species, but I hope this motivates scientists to question the “fashionable” explanation of “global warming” and actually do some serious scientific investigation, like this team did. If so, real science might still be able to help us understand (and the hopefully fix) the problem.
Not long ago, I wrote a post about the COVID-19 vaccine produced by Pfizer. At that time, I only had access to the results of the small clinical trial, but those results were very encouraging. Now, the initial results of the large clinical trial are available, and they are even more encouraging. In short, the vaccine is 95% effective at preventing symptomatic cases of COVID-19 in the group that was being tested. While there were side effects, they were generally mild. Of course, not all kinds of people were tested. People under 16 years of age were not included in the clinical trial. Neither were pregnant women nor those who are immunocompromised. Thus, the results don’t apply to people in those groups.
Like most clinical trials used for licensure of a medication, this was a large-scale, placebo-controlled, double-blind study. That means a large number of people (43,538) were randomly assigned to receive either two doses of a placebo (an injection of saltwater) or two doses of the vaccine. The doses were separated by 21 days. Neither the people getting the injections nor the researchers directly involved in the study were aware of which injection each person got (that’s what “double blind” means). Once there were enough COVID-19 cases among all the participants to make a reasonable conclusion about the results, the researchers learned which injection each participant got. At that point, they could compare the two groups.
When they made the comparison, they found that starting seven days after the second dose, there were only 8 cases of COVID-19 in the group that got the vaccine doses, while there were 162 among those who got the saltwater injections. Thus, the vaccine clearly provides strong protection against COVID-19, at least among people like those who were in the study. Now please understand that people in the study were only tested for COVID-19 if they exhibited symptoms, so this says nothing about whether or not the vaccine protects against asymptomatic COVID-19 infections.
Of course, the small clinical trials had already shown that the vaccine would be effective at preventing symptomatic cases of COVID-19. This large-scale trial was done to confirm that result and, more importantly, to determine whether or not the vaccine is safe for the majority of people. While it is impossible to know for sure, all indications are that for people over 16 who are not pregnant and not immunocompromised, the vaccine is safe. The vast majority of vaccine recipients reported pain at the injection site, compared to only a small percentage of those who got the placebo. Small percentages of those who got the vaccine also reported redness and swelling at the injection site.
The most commonly-reported side effect after pain at the injection site was fatigue. In people aged 16-55, for example, 59% of those receiving the vaccine reported fatigue after the second dose, compared with 23% of those who got the placebo. The percentages were slightly lower for those over 55. Headache was the next most common side effect, followed by muscle pain, chills, joint pain, fever, diarrhea, and vomiting. Figure 2 from the study gives a good summary. There were a total of four people who had severe reactions to the vaccine. Those reactions were a shoulder injury related to administration of the vaccine, severely swollen lymph nodes, an abnormal heart rhythm, and unexplained severe sensations in the leg. There were two vaccine recipients who died, but there were four placebo recipients who died. None of the deaths were judged to be related to the clinical trial.
Based on these results, I plan to get the vaccine as soon as I am allowed to. My wife is in a high-risk group, and she will as well. My adult daughter and her husband have a business that requires extensive travel throughout the U.S. They will also be getting it. Whether or not you or your family get this vaccine (or one of the others that will no doubt become available over time) is up to you. Medical decisions are deeply personal and should be made in consultation with a physician who knows your medical history. I would never presume to tell anyone how to make such decisions. I simply wanted to communicate to my readers what I think the data say about this vaccine.
I will add one more thing. One of my readers said that she heard the COVID-19 vaccine can make women unable to have babies, because the vaccine is training the body’s immune system to fight a protein that is similar to syncytin-1, a protein important to the formation of a placenta. Thus, it is possible that a woman who gets pregnant after getting the vaccine will be unable to form a placenta. While it is true that the proteins are similar, their similarity is in their function, not their actual structure. Both proteins facilitate connection to a membrane, but they do so in very different ways. As a result, their structures are quite different, and a protein’s structure is what the immune system attacks. Thus, there is no reason to expect that the vaccine will cause the immune system to attack syncytin-1.
In addition, women who contract the actual disease would have the same problem, since the immune system attacks the same protein whether it comes from the instructions given by the vaccine or the virus itself. I don’t know of any reports indicating that women who contracted COVID-19 are unable to form a placenta. Finally, while pregnant women were excluded from the trial, 23 got pregnant during the trial. Twelve of them were in the group that got the vaccine. They are being followed, and as of the December 4th National Vaccine Advisory Committee meeting, no adverse effects have been found.
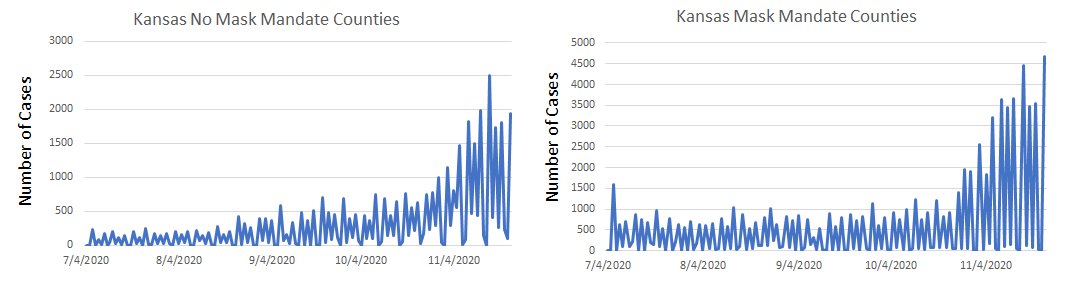
Comparison of COVID-19 cases in Kansas Counties that adopted a mask mandate on July 3 and those that did not. (click for higher resolution)
My previous post discussed two studies that seem to indicate masks have little effect when it comes to stopping the spread of COVID-19. I had several Facebook commenters who disagreed with my interpretation of the studies, which is not surprising. One commenter linked a recent study promoted by the CDC, which makes the remarkable conclusion that in Kansas, counties that adopted a mask mandate saw a 6% decrease in new cases, while those that did not adopt the mandate saw a 100% increase. If true, that indicates masks have a strong effect when it comes to stopping the spread of COVID-19. After reading the study and doing my own analysis of the numbers, I have to say that unfortunately, it is not true.
Once again, let me preface this by saying that I am not anti-mask. I wear a mask whenever I am in public, and I did so even before my state made it mandatory. In addition, I am not telling people to stop wearing masks. As I said in my first post, any mask not made specifically for viruses will be pretty much worthless in protecting the wearer. However, a mask does reduce the number of water droplets that the wearer spews into the air, and since those droplets can contain viruses, it probably does protect the people around the wearer, albeit to a small extent. Thus, you should wear a mask. At the same time, however, you need to have a realistic idea of what kind of protection it provides. So far, the data say it offers only a little protection.
With that out of the way, let’s look at the study. It examined various counties in Kansas that adopted a mask mandate on July 3, 2020 and compared them to the other counties that did not adopt a mask mandate. It developed a seven-day rolling average of new COVID-19 cases for both sets of counties and compared the numbers before July 3 and After July 3. The graph (shown near the bottom of the study) shows that while the 7-day rolling average continued to climb for those counties that did not adopt a mask mandate, it fell a bit for those counties that did. Thus, the mask mandate actually reduced COVID-19 cases, while lack of a mandate resulted in a steady increase in cases.
A surgical mask like the ones used in the study being discussed (click for credit)
In the midst of this pandemic, most governments are requiring people to wear mask in public. I will start this by saying that I began wearing a mask early on in the pandemic, long before any mandates were made. I didn’t wear one because I thought it would be effective. Even a basic understanding of science tells us that standard masks provide little protection against the spread of a virus. Protecting yourself against a virus using a mask that is not made specifically for viruses is roughly equivalent to protecting your yard against mosquitoes by installing a chain-link fence.
However, a mask does reduce how many water droplets you spew into the air, and since those droplets can carry viruses, there is probably some small protective effect for those with whom you come into contact. I wore a mask early on simply to put others at ease. Now I wear one because I think people must follow a society’s rules (unless they are immoral) in order to be a functional member of that society. If the mandates were lifted, however, I would still wear a mask in public until the pandemic dies out, simply because some people think it protects them, and I want to put such people at ease.
Having said that, there has been one study that concluded mask mandates reduced the rise of COVID-19 infections by a tiny amount. However, the study couldn’t conclude that the masks were the cause of the tiny decline. Most likely, when a mask mandate is instituted, people become naturally more cautious, limiting their social interactions, being more aware of social distancing, etc. Thus, it’s possible that the masks had nothing to do with the small reduction in COVID-19 cases.
My publisher sent me a recent study that tries to address the question a bit more effectively than the study linked above. It didn’t test masks directly, because it would be impractical to follow people around making sure they were wearing their masks. However, the study gave 3,030 people a set of recommendations for protecting themselves against COVID-19. They included things like social distancing, etc., as well as the recommendation to wear a mask, 50 surgical masks, and instructions on how to use them. The study also gave 2,994 people the same set of recommenstions, minus the mask recommendation, the masks, and their instructions. After 1 month, they tested people for COVID-19 antiboides. This was all during a time when their communites did not issue any mask recommendations or mandates.
The results showed that slighly fewer people in the mask group contracted COVID-19 than those in the no-mask group. However, because the number of people who contracted COVID-19 during the study was small, the difference between the groups could have been the result of random chance. In the end, the authors use basic statistics to conclude that the mask group was somewhere between 46% less likely to get the disease and 23% more likely to get the disease. As they say:
The recommendation to wear surgical masks to supplement other public health measures did not reduce the SARS-CoV-2 infection rate among wearers by more than 50% in a community with modest infection rates, some degree of social distancing, and uncommon general mask use. The data were compatible with lesser degrees of self-protection.
Now, of course, we have no idea what percentage of the people in the mask group actually followed the recommendation, but the study made it pretty easy to do so. Combined with the study I linked at the beginning of the post, I think we can conclusively say that if the typically-used masks provide protection against COVID-19, it is small. Thus, when “experts” say nonsense like this:
If we could get everybody to wear a mask right now, I really think in the next four, six, eight weeks, we could bring this epidemic under control.
We know they are not using science to inform their opinion.
Pfizer’s description of how an mRNA vaccine works (click for larger version)There has been a lot of talk about Pfizer’s COVID-19 vaccine, and a reader asked me to comment on it. The company claims it is more than 90% effective at preventing the disease, which is better than what most health-care experts were expecting. If true, that news is exciting enough. To add to the excitement, it is a new kind of vaccine that has great potential, if it works the way it is supposed to. There is another company trying to produce a similar vaccine, but it looks like Pfizer is in the lead, so for the purpose of this article, I will focus on its version.
Let me start by saying that I have no connection to Pfizer or any other pharmaceutical company. I am a science educator who writes about science issues like this one. I am also not a medical doctor or medical researcher. I am simply a nuclear chemist who has broadened my knowledge base by writing (or co-writing) a series of textbooks used by home educators and teachers in Christian schools. Thus, I am no expert on these matters. However, I get most of my information by reading the scientific literature, which allows me to avoid a lot of the misinformation found in the standard media outlets and (even worse) social media.
Before I talk about Pfizer’s vaccine in particular, I want to explain how this kind of vaccine works. To understand that, remember that a traditional vaccine uses a weakened/inactivated form of the pathogen whose infection it wants to prevent (or a chemical mimic of that pathogen). This causes your body to react as if it is being infected by the real thing. As a result, it mounts a defense that is specific to that pathogen and remembers how to fight it. That way, if you get infected by the real thing, it can mount a swift immune response. This process takes advantage of your acquired immune system. However, you also have an innate immune system, and the active ingredient of the vaccine does not stimulate it. As a result, traditional vaccines have additives, called adjuvants, which are designed to stimulate your innate immune system. That way, everything in your immune system works the way it is designed to work.
Carbon dioxide absorbs the infrared radiation that the earth emits, trapping it before it leaves the planet. This warms up the atmosphere, making the earth a haven for life. Obviously, then, the more carbon dioxide we put into the atmosphere, the warmer it will get, right? Not necessarily! As I tell my high school and university students over and over again: Science isn’t simple! As a result, conclusions that seem “obvious” to most people (even most scientists) are often absurdly wrong. A recently-produced study that has not yet been published in the peer-reviewed literature makes this case about carbon dioxide and global warming, aka “climate change.”
The “obvious” conclusion that more carbon dioxide means more global warming ignores the fact that carbon dioxide doesn’t absorb all the infrared radiation it encounters. Instead, it only absorbs specific wavelengths. In addition, the amount of each wavelength that carbon dioxide can absorb varies with wavelength, the temperature at which the absorption happens, the concentration of the gases in the surroundings, etc., etc. Because of such effects, there comes a time when adding more carbon dioxide to the atmosphere has a negligible effect on the amount of infrared radiation absorbed. When that happens, you have reached saturation, and increasing the amount of carbon dioxide will not increase the atmosphere’s warming.
Now all of this is well known, and most global warming models attempt to include these effects in their calculations. The problem is that they treat them in a crude way. This is understandable, since a model that is trying to simulate the entire atmosphere has to consider a lot of things. As a result, most of them are treated crudely so that the model doesn’t become overwhelmingly convoluted. That’s where this unpublished study comes in. The authors test the effect of treating the science related to saturation crudely, and they say it renders the models pretty much useless when it comes to understanding how carbon dioxide affects the present atmosphere.
How do they come to this conclusion? They consider more than 300,000 different infrared wavelengths that carbon dioxide and other greenhouse gases (water, ozone, methane, and dinitrogen oxide) absorb. They compute how much the gases will warm the atmosphere by absorbing each wavelength. First, they make the computation without considering details like the temperature, the other gases in the atmosphere, etc. This is roughly equivalent to how current models treat the situation. Then, they do it considering all those details, using the present makeup of the atmosphere. They find that in the present atmosphere, the amount that more carbon dioxide can contribute to global warming is 10,000 times smaller than what current models assume. The same can be said for water vapor. For carbon dioxide and water vapor, then, the atmosphere is very, very close to saturation. As a result, more carbon dioxide and water vapor in the atmosphere will not warm the planet in any meaningful way. Ozone, dinitrogen oxide, and methane are also close to saturation, but not nearly as close as carbon dioxide and water vapor.
How do we know that their analysis is correct? We don’t. When they compare their calculations of how much infrared radiation is being absorbed for each wavelength to what satellites have been measuring, they see virtually no difference. Thus, their calculations seem to reflect reality very well. However, I am not very knowledgeable about the details, so there might be fatal flaws in their analysis that I am not seeing. Once again, science isn’t simple. I really hope this gets published in the peer-reviewed literature so that experts can weigh in on the conclusions. Unfortunately, I am not confident this paper will get that far. If its conclusions are correct, then there is absolutely no basis for the fear-mongering that surrounds carbon dioxide emissions. There are so many scientists whose careers have been made based on that fear-mongering, they may simply keep the paper from being published.
Fortunately, science is self-correcting. One way or another, we will figure out the details related to this issue. It might take longer than it should, and it might be after terrible decisions have been made based on faulty climate science, but at some point in the future, we will find out whether or not these authors are correct. I hope it is sooner rather than later!
Three months ago, I blogged about an excellent article which used statistical methods to demonstrate that the fine-tuning seen in biology is even more extreme than what is seen in the properties of the universe as a whole. It was very much supportive of intelligent design and referenced many works from the intelligent design community. The article, which was published in a secular, peer-reviewed journal, finally caught the notice of the Inquisition. As a result, the High Priests of Science demanded penance from the editors of the journal. Their penance has come in the form of a disclaimer that appears in the journal. Here is what the disclaimer says:
The Journal of Theoretical Biology and its co-Chief Editors do not endorse in any way the ideology of nor reasoning behind the concept of intelligent design. Since the publication of the paper it has now become evident that the authors are connected to a creationist group (although their addresses are given on the paper as departments in bona fide universities). We were unaware of this fact while the paper was being reviewed. Moreover, the keywords “intelligent design” were added by the authors after the review process during the proofing stage and we were unaware of this action by the authors. We have removed these from the online version of this paper. We believe that intelligent design is not in any way a suitable topic for the Journal of Theoretical Biology.
I laughed out loud when I read this, because it shows how ignorant the journal editors are when it comes to the issue of origins. As a bonus, it also shows how wrong the High Priests of Science are about intelligent design and creationism.
First, the disclaimer makes it clear that the journal editors know nothing about intelligent design. Anyone with even a passing knowledge of intelligent design and the work that has been done in the area would immediately recognize that this paper strongly supports intelligent design. Yet the journal editors didn’t seem to notice at all! Thus, this very disclaimer is admitting that the journal editors are against something they know virtually nothing about!
Second, the disclaimer shows how strong the science in the article is. After all, the journal is predisposed to dislike any science that points to intelligent design. Nevertheless, this article points to intelligent design, even if the editors are too ignorant to realize that. Thus, the evidence it presents is so strong that even some scientists who are predisposed to be against its conclusions consider it worthy of publication!
Third, they note that while the authors “are connected to a creationist group,” their addresses are from “bona fide universities.” Why? Because creationists and intelligent design scientists are real scholars. “Bona fide universities” would not hire non-scholars! So even though the High Priests of science dogmatically say that those who support intelligent design aren’t real scholars, this very disclaimer admits that they are!
The disclaimer shows the untenable situation in which science finds itself today. The High Priests of Science proclaim from their exalted places of power that intelligent design and creationism aren’t science. Nevertheless, their actions demonstrate the exact opposite. This untenable situation cannot last, and when it finally does collapse entirely, science will be much better off.
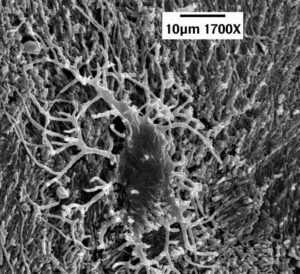
The dark mass near the center is the cell body of a dinosaur bone cell. The various “arms” extending from the body are its filipodial extensions. (click for credit)I have written a lot about soft tissue found in dinosaur fossils and other fossils that are supposed to be millions of years old (see here, here, here, here, here, and here, for example). Right now, the best work being done on this issue comes from the Dinosaur Soft Tissue Research Institute, which is run by microscopist and young-earth creationist Mark Armitage. Without the help of government grants, he and his colleagues have produced some truly incredible work. Their latest contribution was published in Microscopy Today, and it strengthens the case that these fossils cannot be millions of years old. As always, I encourage you to read the article in its entirety, but here is my “color commentary.”
First, the article shows more incredible, delicate structures that would not be expected to survive any preservation process that would protect them for millions of years. For the first time in the scientific literature, there are two excellent pictures of dinosaur vein valves (Figures 2 and 3), features that are so delicate they are hard to extract from animals that have just recently died. In another first, he shows a nerve from the same fossil (Figure 6). In that nerve, you can see the delicate Bands of Fontana, structures that are unique to nerves.
He also shows a bone cell from the same fossil (Figure 7). While bone cells from dinosaur fossils have been published in the scientific literature, this particular one is very important. Bone cells have characteristic structures called filipodial extensions that are remarkably thin (widths of less than 200 billionths of a meter). The bone cell shown in their study has a filipodial extension that is 24 millionths of a meter long. That doesn’t sound like much, but it is about 30% longer than any other dinosaur filipodial extension found in the literature. This is important, because its length is more than 100 times its width. Think about a structure with those dimensions made out of soft tissue. It would be ridiculously fragile, yet there it is in a dinosaur fossil!
Second, and more importantly, he shows that the current explanation evolutionists have for the preservation of soft tissue in dinosaur fossils doesn’t work. Dr. Mary Schweitzer was the first to give strong evidence for the existence of soft tissue in dinosaur fossils, but she is committed to an evolutionary view. As a result, she needs to find an explanation for how such tissue could survive for millions of years. Seven years ago, she published a study in which she hoped to show that iron from the blood of a dinosaur could produce certain reactions that would preserve the tissues. I wrote about her explanation at the time and how it didn’t seem to make sense based on what we knew. Later on, better chemists than I wrote a detailed analysis about how her explanation is inconsistent with the data.
This new paper demonstrates rather conclusively that Schweitzer’s explanation doesn’t work for the fossil being discussed. Armitage and his colleague (Jim Solliday) search the filipodial extensions of bone cells that are found right outside a canal that held a blood vessel. Since the cells are so close to what was a blood vessel, and since the filipodial extensions are so delicate, those iron-induced reactions should produce noticeable effects on the filipodial extensions. He shows that those effects are not present. Thus, it is unlikely that such reactions happened at all in the fossil.
Also, in her study, Schweitzer took great pains to prevent blood clotting so that iron from the blood could be distributed throughout the soft tissue she was trying to preserve. However, Armitage and Solliday present strong evidence for massive blood clotting in their fossil. This would prevent iron from being able to promote any tissue-preserving reactions. While their evidence is strong, however, it is not conclusive. Thus, as they suggest, more research needs to be done.
The Dinosaur Soft Tissue Research Institute is on the forefront of this issue in science, and they are doing it without the massive government grants available to organizations who are desperately trying to fit the data into an evolutionary framework. If you have the means, I suggest that you make a donation to keep science progressing in this area.
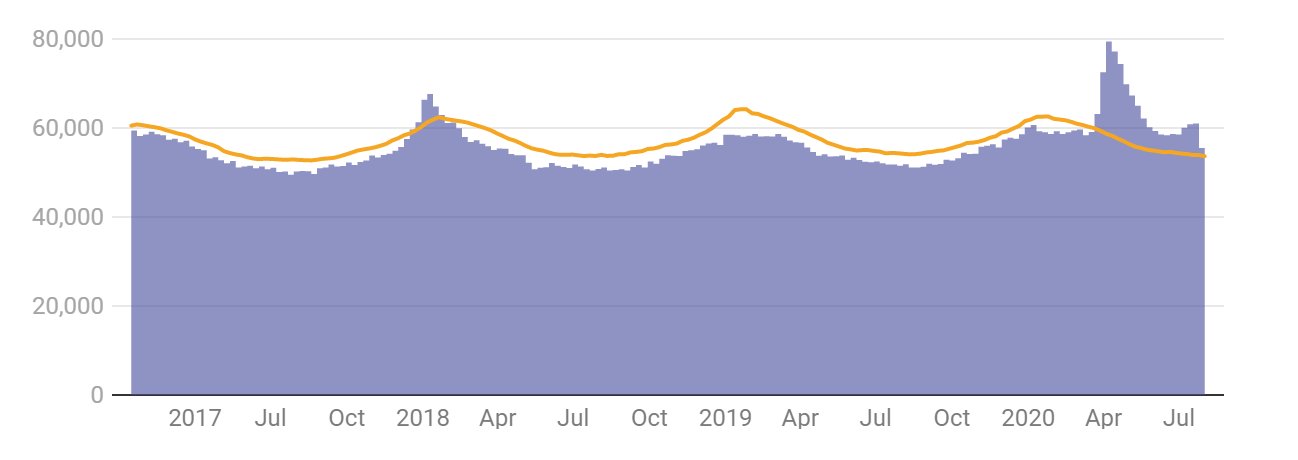
The purple bars are the deaths in the U.S. each week since2017. The yellow line represents the maximum number of deaths that were projected for those weeks. (graph by The Conversation, data from the CDC)
I have referenced this article in some comments I made previously, but I want to highlight it in a separate post, because the graph it contains (also shown above) makes it clear that the COVID-19 deaths are not some manipulation of the data. They are real. Very real. The purple bars in the graph represent all deaths recorded in the U.S. each week since 2017. The yellow line represents a projection of the maximum number of deaths that should have happened each week. The projection is based on historical data, and it fluctuates with the season. That’s because there are usually more deaths in the winter and fewer deaths in the summer, and as you can see, the actual deaths show that same fluctuation.
Notice that for most weeks, the actual deaths were lower than the maximum number of projected deaths. That’s expected. If the projection is done well, there should rarely be a time when the actual number of deaths meets or exceeds the maximum projection. However, there were some weeks in December of 2017 and January of 2018 when that happened, because there was a particularly virulent strain of the flu that season. As a result, more people died than were expected.
But those excess deaths are dwarfed by the ones that start showing up the last week of March in 2020. In that week, about 4,000 more than the maximum projected deaths occurred. Since then, the actual deaths have exceeded the maximum projected deaths by a considerable margin every week. All of this is discussed in the article from which I took the graph. However, I want to make a couple of additional points.
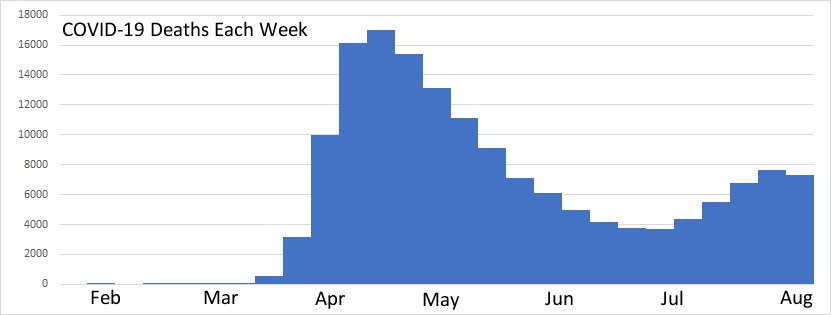
First, look at the shape of the excess deaths. There appear to be two peaks – one very large one the second week of April, and a smaller one at the end of July. This is important, because it looks very, very similar to the COVID-19 deaths reported over the same time span:
When the excess deaths have essentially the same time profile as the COVID-19 deaths, you know that the COVID-19 deaths make up most of the excess deaths. This tells us that the vast majority of COVID-19 deaths are real and most certainly represent people who would not have died had there not been the COVID-19 pandemic.
Second, some friends have asked me why they don’t know anyone who got the disease or died from it. After all, if there really have been more than 180,000 people who died from the disease and more than 6 million confirmed cases, shouldn’t everyone know someone who has suffered from it? Of course not! There are 328.2 million people who live in the U.S. That means about 2% of the population has contracted COVID-19, and about 0.05% have died from it. Thus, your chance of knowing someone who died from it is ridiculously low. While your chance of knowing someone who contracted it but didn’t die from it is significantly higher, remember that for most cases, the disease is mild. Thus, you would have to know someone well enough that you track his or her common illnesses to be aware that he or she had the disease!
It disturbs me that there are so many people (many of whom are Christians) who think this pandemic has been made up. The data clearly say that it hasn’t been. Lots of people died because of the disease, and misinformation will only increase the number of deaths. Now please understand that I am not saying that I support any of the measures that governments have taken to slow the spread. We don’t know enough about the disease or the consequences of the actions that have been taken to know whether or not they are a good idea. I said this before, and I will say it again:
As a scientist, let me assure you that no one really knows what we should be doing. There are a lot of experts saying a lot of different things, and you should listen to all of them. Then, you should decide what works best for you and your family, and you should start doing it. But once you decide what you and your family should be doing, please please please show grace to those who choose to do something different. Since the experts can’t agree on a proper course of action, there is no reason to expect your neighbor to agree with your course of action.
In addition to showing grace to others, please please please stop spreading the false idea that the COVID-19 deaths are few in number or not real at all. They are real, and there are a huge number of them. There is simply no other way to understand the data.
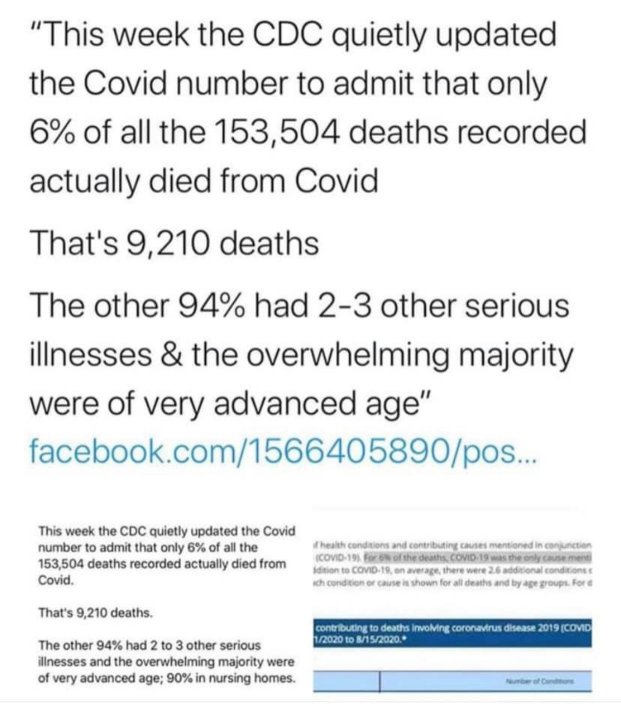
Falsehoods meant to downplay the seriousness of COVID-19 (click for an enlarged image)On Saturday, I received the image on the left from a well-meaning individual. She wanted me to see that we have been fooled regarding the severity of the virus that causes COVID-19. By Sunday, this image (or one like it) was all over my Facebook feed. Please understand that the statement starts out as completely false and then uses true statements to imply something else that is completely false. Unfortunately, it tends to resonate with people who do not understand medical science and who have not been personally affected by the pandemic. As I watched this lie literally spread around the world, I couldn’t help but think of Jonathan Swift’s famous statement1
Falsehood flies, and the Truth comes limping after it.
Here is my attempt to get the truth to come limping after this falsehood.
More importantly, this image is meant to imply that COVID-19 is not dangerous because the vast majority of people who die from it have some other illness. Once again, that is simply 100% false. If you look at the underlying conditions that are included in the 94% (table 3 in the link above), you find things like high blood pressure (hypertensive diseases), diabetes, obesity, etc. The image tries to categorize them as “serious illnesses,” and depending on the person, they might be. However, they are present in a large percentage of the population. 45 percent of adults in the U.S. have a hypertensive disease, 10 percent of the U.S. population have diabetes, and 42 percent have obesity. Thus, a huge number of people in the U.S. have at least one of the “serious illnesses” that make you likely to die from COVID-19. In other words, there are many, many people at risk of death from COVID-19.
But how can we say that these people died of COVID-19 when they had some other condition? Because most of these conditions are completely treatable and will not generally kill a person. However, when that person gets an infection, the underlying condition makes it harder for his or her body to fight off the infection, leading to death. The more serious the infection, the more likely the person is to die. In fact, the majority of people who die of an infection like influenza, pneumonia, tuberculosis, etc. have an underlying condition that makes it more difficult for them to fight off the infection. Thus, it is not even remotely unusual that 94% of people who die from COVID-19 had one or more underlying conditions. It is common for many serious infectious diseases, especially in the developed world.
There is one more issue in the image above that I must address. It says that the overwhelming majority of people who died from COVID-19 were of advanced age. That’s true, but it’s true for all deaths in the developed world, not just COVID-19 deaths. Indeed, a recent study compared the ages of people who died from COVID-19 to those who died from all causes. Guess what? They were quite similar:
In fact, the age distribution of deaths attributed to COVID-19 is quite similar to that of all-cause mortality, which tends to increase by about 10% every year of age after age 30 y.
We don’t know a lot about COVID-19, and there is no way to scientifically state the best cause of action against the disease at this time. However, we do know that it is a very serious disease, and it is being downplayed by some using falsehoods like the image above. Please stop the misinformation! If you want to share something about COVID-19, at least make sure it doesn’t communicate something blatantly false, like the image above does.
ADDENDUM (added 9/4/2020): Someone on a friend’s Facebook feed wrote an incredibly insightful comment that I must share. She said that if you really think that the only COVID-19 deaths are the ones that had COVID-19 as the sole cause, then you must think that AIDS has a mortality rate of zero!
REFERENCES
1. The Examiner, Number 15 November 2 to November 9, 1710, (Article by Jonathan Swift), Page 2, Column 1, Printed for John Morphew, near Stationers-Hall, London. Return to Text
_(21602909135).jpg)



 Carbon dioxide absorbs the infrared radiation that the earth emits, trapping it before it leaves the planet. This warms up the atmosphere, making the earth a haven for life. Obviously, then, the more carbon dioxide we put into the atmosphere, the warmer it will get, right? Not necessarily! As I tell my high school and university students over and over again: Science isn’t simple! As a result, conclusions that seem “obvious” to most people (even most scientists) are often absurdly wrong.
Carbon dioxide absorbs the infrared radiation that the earth emits, trapping it before it leaves the planet. This warms up the atmosphere, making the earth a haven for life. Obviously, then, the more carbon dioxide we put into the atmosphere, the warmer it will get, right? Not necessarily! As I tell my high school and university students over and over again: Science isn’t simple! As a result, conclusions that seem “obvious” to most people (even most scientists) are often absurdly wrong. 
{kind=link}